From the desk of the CEO…
Today we announced our $150 million Series-E, led by Goldman Sachs, bringing our total funding to over half a billion dollars.
This is a significant milestone for Aidoc and the industry, reflecting the growing momentum in the field of Clinical AI. It also reflects an ongoing commitment to the hospitals and physicians we work with who are navigating the most demanding era in the history of medicine.
But… I don’t want to start with the funding. I want to begin with a statement that has driven us for the past nine years:
Healthcare is now facing the largest public health crisis in history, and we finally have the tools to do something about it.
For nine years, we have been driven by a single reality: healthcare is facing a systemic crisis. The AAMC projects a shortage of up to 86,000 physicians in the U.S. by 2036 and clinicians are feeling the weight of this deficit today.
Radiology is particularly acute: imaging studies have grown by up to 5% per year in recent years, far outpacing the growth of radiology residency positions.
When the system is stretched this thin, clinicians face an unsustainable cognitive load, leading to burnout and, tragically, increased diagnostic errors.
Data from Johns Hopkins University underscores the costs of systemic pressure we collectively face: an estimated 900k Americans are killed or permanently disabled each year by diagnostic errors.
That’s approximately 420,000 deaths and 480,000 people left with permanent disabilities: paralysis, brain damage, organ failure and more. To put that in perspective: the total number of American deaths in World War II was about 420,000. We are losing the equivalent of an entire wartime generation every year to a mostly preventable problem.
We have incredible clinicians and the best healthcare in the world, for which we have to be thankful. But… the system is stretched beyond recognition.
If we do nothing, these problems get worse.
We have to augment diagnostic safety and capacity.
With no obvious miracle solution to healthcare’s labor shortage, we need a new paradigm. One with AI at every care encounter. An extra layer of support that lets clinicians deliver the care they want for their patients.
The beginning
After the Allied victory at El Alamein, Churchill famously said: “Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.” I believe we’ve now officially crossed into the end of the beginning for clinical AI.
The first chapter for clinical AI has been focused on scaled adoption. It requires solving two major issues:
- Building models accurate and safe enough for clinician use
- Scaling them to drive real impact
Building clinical AI models in itself is an incredible undertaking.
Creating a model that was accurate enough to support physicians took blood, sweat and tears.
Although the deep learning revolution made it possible to even tackle this problem, there was a tradeoff. You could only solve one problem at a time. The model was straightforward, with complex execution: focus on a condition where AI could make a big impact, develop a model, get FDA clearance, and deploy. One condition at a time.
But creating great AI models was only part of the challenge. To implement them at scale, we needed to build the infrastructure to support their operation.
This is what motivated us to create aiOS, our clinical AI operating system.
Think of it this way: every AI solution was like a show on Netflix. Some shows were amazing. But Netflix didn’t exist yet so people couldn’t see them. We had to build the streaming platform first.
And after what seemed to be a sisyphean task, it worked. AI is now embedded in the standard of care. Across thousands of hospitals, our solutions have helped ensure that tens of millions of patients get the accurate and timely care that they deserve. In some cases, we’ve seen a reduction in time to diagnosis of 98% for incidental pulmonary embolism in the outpatient setting, from over 5 days to under 90 minutes.
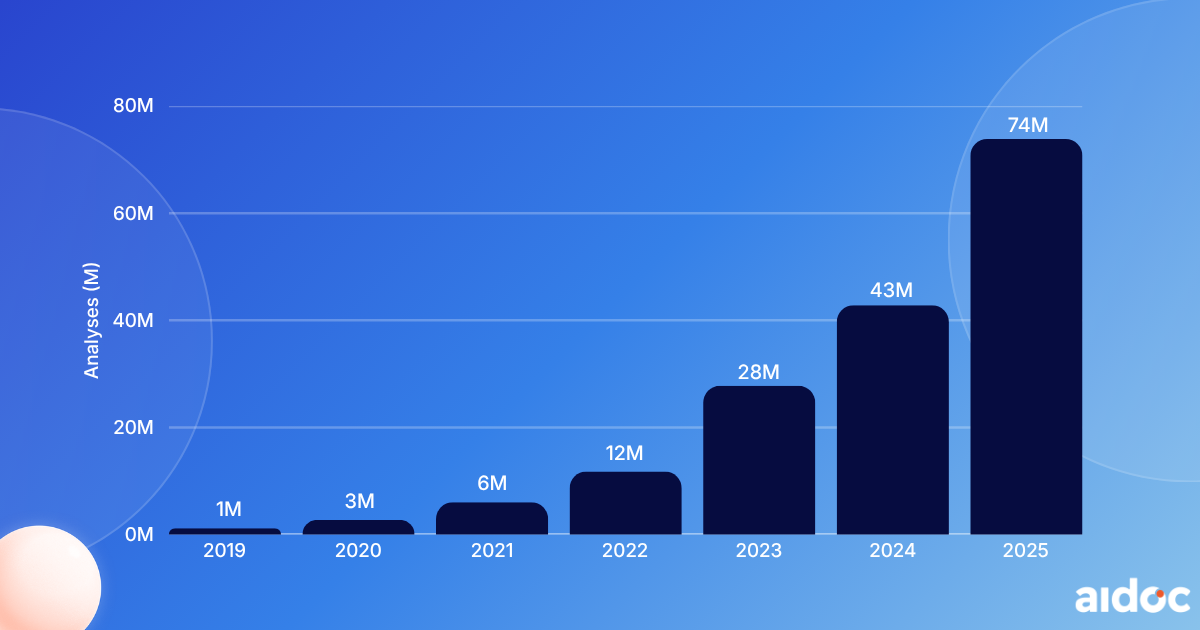
And we’re growing exponentially: last year, we exceeded 60 million AI patient cases annually and now operate in nearly 200 health systems. Partners that begin with Aidoc today implement AI across an average of 12 conditions, up from just 2-3 a few years ago.
This transformation is only possible thanks to tech progress (aiOS supporting it) and incredible healthcare leaders embracing change and pushing for adoption.
Clinical evidence on the use of AI spans more than 200 published studies. The results are real.
Market Adoption: Annual AI Patient Cases Analyzed
But still, the scope of the problem made it clear that we needed to do more. We still received daily calls from health system CEOs and clinicians describing the challenges from the front lines.
Our next chapter: two new frontiers
The next chapter builds on the infrastructure from “the beginning” and unlocks two new frontiers. Solving each is a huge undertaking unto itself, but together they combine to create a major leap forward for medicine.
The first is creating a ubiquitous safety net, to support every care encounter. The second is easing the capacity crisis, to help clinicians do dramatically more with the time they have.
This is what motivated us to create CARE.
Frontier 1: A ubiquitous safety net, with foundation models
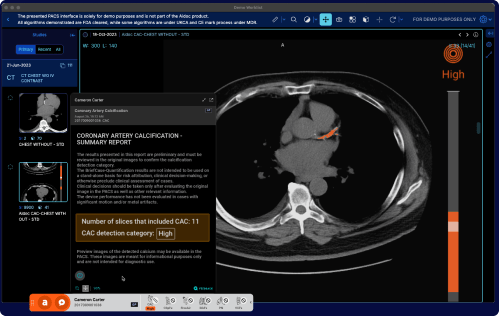
CARE is Aidoc’s clinical-grade foundation model, built on our own architecture and trained on years of real-world clinical data.
CARE allows us to rapidly develop clinical AI: instead of training models one condition at a time, CARE creates a shared intelligence layer that quickly expands across various pathologies and diagnostic tasks. With CARE, in just a few months we have already doubled our disease coverage.
The CARE Inflection: FDA Cleared Solutions Available Over Time

Building a foundation model is an immense undertaking both in compute and R&D resources (which is why this round was essential). But speed alone isn’t sufficient. It has to be paired with safety.
CARE allows us to make a major leap in performance, demonstrating a tenfold reduction in false positives/negatives compared to earlier iterations, providing the high-fidelity support required for acute care decisions. It marks a shift to clinical AI infrastructure that health systems can manage, expand, and rely on.
Seatbelts are not a luxury
Despite this progress, we can learn from the lessons of history; adoption isn’t always linear.
In the mid-twentieth century, as Americans increasingly took to the roads in private cars, tens of thousands were dying in car crashes. In 1959, Nils Bohlin developed the seatbelt; but it took until the mid-80s before seatbelts were widely adopted, and the USA saw a 75% decrease in automobile deaths. Today, seatbelts, airbags, and other safety measures are accepted as the standard.
I believe clinical AI in every encounter is an inevitability.
Soon, practicing medicine without AI will become as unthinkable as driving without a seatbelt.
Safety with clinical AI is a win-win-win
For clinical AI to be ubiquitous it has to be good for “the P’s of healthcare”: patients, providers, and practices.
For patients, whether you get great care still depends too much on where you live and who’s available when you need them. AI unlocks access to timely, high-quality care for everyone. It sets a new, higher standard of care.
For providers (clinicians), AI frees them up to do their best work; faster, more easily, and with the confidence of an “always on” clinical copilot. This means better, more efficient workflows, with less cognitive burden for them and better quality care for patients.
For practices (health systems), technology has to be sustainable. AI that improves quality of care mitigates leakage, drives more appropriate care, helps control costs and increases throughput.
Leveraging clinical AI to improve clinical care is good for patients, game-changing for clinicians, and has a positive downstream impact for health systems.
Frontier 2: Easing capacity, with report drafting
CARE addresses the safety net. The second frontier is capacity. Imaging volumes keep climbing, residency slots cannot keep up, and radiologist turnover has roughly doubled over the past decade. We cannot hire our way out of this.
The next leap is AI that takes the findings detected, and actually drafts. What Cursor (or Claude Code, or Copilot, pick your poison) is doing for software engineering, we need to do for medicine.
We are building AI-generated draft reporting. It produces a preliminary radiology report directly into the radiology reporting systems. Radiologists review, edit, and attest. Not a replacement for clinical judgment. A multiplier on it.
But drafting demands a higher bar on detection. Generating a report is a far higher-stakes task, and it has to be built on a deep infrastructure of safety and quality. Consistent model accuracy will matter more than ever.
If CARE is the safety net, CARE Reporting is the accelerant.
What will we do with the $150 million? Simple: invest heavily in R&D
Much of that investment is directed toward CARE: expanding tasks and disease coverage. We want to cover hundreds of diseases in the next couple of years.
aiOS similarly will have to undergo major upgrades to scale. Improved analytics, governance tools, and more advanced downstream multi-modal integration.
Of course, AI-generated draft reporting will be a significant investment as well.
Above all, we will continue investing in our safety infrastructure. Every solution we build, especially report drafting, is only as valuable as the safety guardrails behind it. The faster we move, the more that discipline matters.
Goldman Sachs will be an incredible partner
They share our passion, and their decision to lead this round is, to me, an unequivocal signal that clinical AI has crossed the chasm: clinical AI has become a standard layer of how health systems operate.
They are joined by General Catalyst, NVIDIA, Softbank, Square Peg, and many other trusted partners who have believed in this mission from the beginning.
To our customers and partners
We started Aidoc because we believed we could use technology to fundamentally change what’s possible in medicine. Not incrementally, but at a scale and pace that truly matches the urgency of the problem.
Today, more than ever, we feel that urgency. We understand you want more. You need more from us.
We appreciate your trust. We recognize you chose us not only for our products but also for our culture, innovation, and future plans. We do not take that trust lightly.
We are dedicated to maintaining the highest standards of safety and quality. We are committed to matching your sense of urgency. We aim high, knowing we need your partnership to succeed.
Onwards.
Elad Walach, CEO
Aidoc’s Series E: The End Of The Beginning – Aidoc | Clinical AI
Discover more from
Subscribe to get the latest posts sent to your email.
